Femoro-acetabular impingement (FAI)
Abnormal contact between the femur and acetabulum which leads to labral damage and various degrees of chondral injury
CAM vs Pincer Effect ( or both)
Clinical symptoms
activity related groin or hip pain, exacerbated by hip flexion
difficulty sitting
mechanical hip symptoms of clicking or popping
can present with gluteal or trochanteric pain
due to aberrant gait mechanics
limited hip flexion (<90 degrees), especially with internal rotation (<5 degrees)
Pain on FADIR maneouvre (flexion, adduction, internal rotation): Generally the affected limb is in externally rotation.
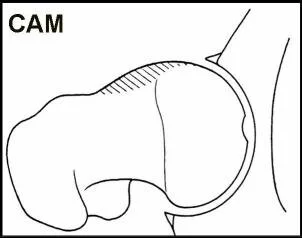
CAM impingement
occurs if femoral head/neck bone is too broad, mostly on the anterolateral neck
usually young athelete male
characterized by any of the following
decreased head-to-neck ratio
aspherical femoral head
decreased femoral offset
femoral neck retroversion
causes shearing at the chondro-labral junction, leading to cartilage delamination and labral separation .
Chondral damage occurs more frequently on the anterior superior portion of the acetabulum.

Grantham, W. J (2019). Etiology and Pathomechanics of Femoroacetabular Impingement. Current Reviews in Musculoskeletal Medicine.
PINCER impingement
occurs if acetabular bone/labrum overhang is too broad, mostly at the anterosuperior quadrant
antero superior acetabular rim overcoverage
acetabular retroversion
acetabular protrusio
coxa profunda
usually in active middle-aged women
the femoral neck impinges and crushes the labrum creating intra-substance tearing
this levers the femoral head into the postero-inferior acetabulum leading to a contrecoup cartilaginous injury


Grantham, W. J (2019). Etiology and Pathomechanics of Femoroacetabular Impingement. Current Reviews in Musculoskeletal Medicine.

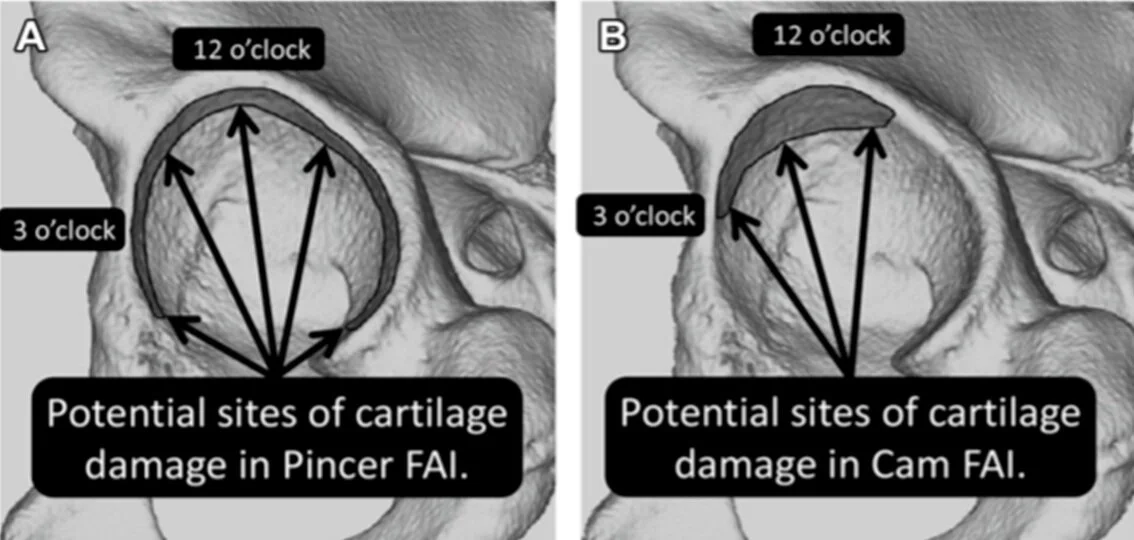
Repartition of cartilage damage in femoroacetabular impingement
Grantham, W. J (2019). Etiology and Pathomechanics of Femoroacetabular Impingement. Current Reviews in Musculoskeletal Medicine.

Difference in labral lesions CAM vs PINCER
Seminars in Musculoskeletal Radiology, 23(03), 257–275. doi:10.1055/s-0039-1683967
Imaging:
Xrays : AP +L + Frog leg (for alpha angle measurement) + DUNN + Lequesne false profile
Must search for the following: Coxa profunda and coxa protrusio, Center-edge angle of Wiberg, Acetabular index, Crossover sign, Posterior wall sign, Ischial spine sign, femoral head sphericity on all views, osteoarthritis
CT scan: 3D is important for pre-operative assessment
MRI for labrum ad cartillage damage assessment.
Prefer Arthro MRI for accurate.
Ensure MRI is formatted to be in-line with femoral neck
Findings: Labral fraying or frank tears, chondral damage, subchondral cyst formation
Arthroscan can replace MRI

DUNN lateral view

False Profile Lequesne: to assess anterior coverage of the femoral head

False Profile Lequesne: to assess anterior coverage of the femoral head

Check the quality of the Xray before judging !!!


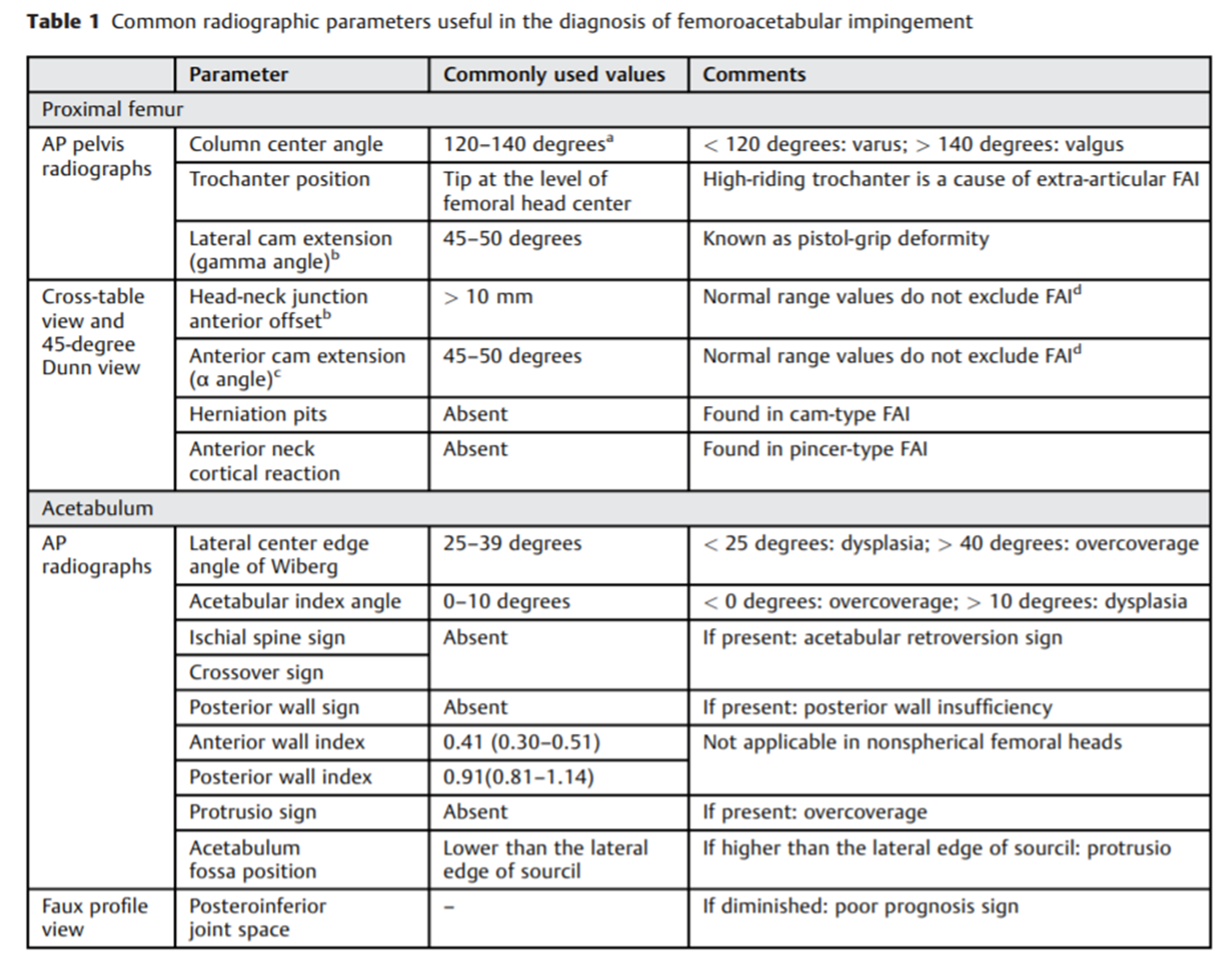
Useful radiographic parameters
Seminars in Musculoskeletal Radiology, 23(03), 257–275. doi:10.1055/s-0039-1683967

Useful MRI parameters
Seminars in Musculoskeletal Radiology, 23(03), 257–275. doi:10.1055/s-0039-1683967


What we find in CAM imaging

CAM impingement

Pistol- grip like deformity

Alpha angle: values of >42° are suggestive of a head-neck offset deformity, >50-55° indicates Cam deformity
Assessed on frog-leg lateral radiograph

Alpha angle on MRI
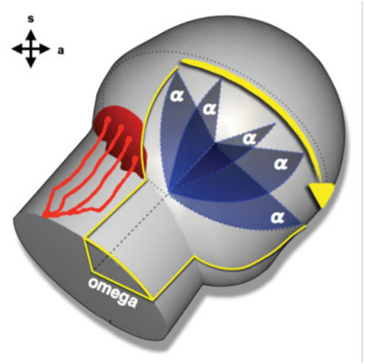
Omega angle

Femoral head neck offset : distance between line 2 (neck line) and 3femoral head line). If <10 mm —> CAM

head neck offset ratio= FHNO/diameter of FH.
If <0.17—>CAM
What we find in PINCER imaging

Lateral center edge angle (or Wiberg angle). Normal between 25-40 degrees

Anterior center edge angle
Normal > 20

Tonnis angle ( Normal above 0 degree)

Cross over sign


Differential Diagnosis: Various pathologies will refer pain to the hip region
hip instability
iliopsoas pathology
Ischiofemoral impingment
adductor strains and athletic pubalgia
lumbar radiculopathy
Treatment
Activity modification, Physical therapy, NSAID
Arthroscopic osteoplasty
Hip arthroplasty (if osteoarthritis)
Complications: heterotopic ossification, femoral neck fracture…