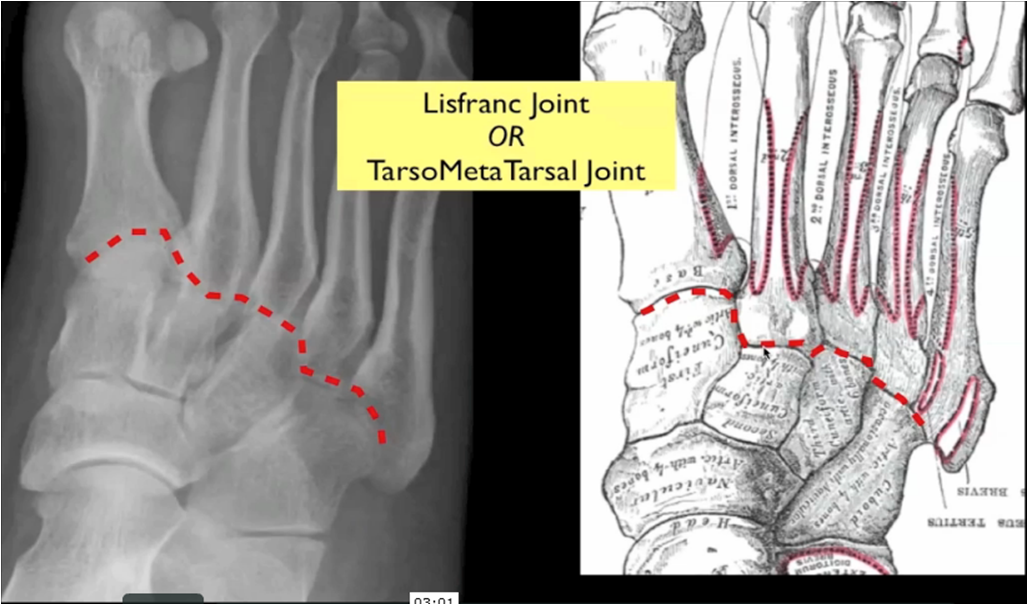
Lisfranc injury
Disruption between the articulation of the medial (1st) cuneiform and base of the second metatarsal à disruption of the TMT joint complex
Injuries can range from mild sprains to severe dislocations. May take form of purely ligamentous injuries or fracture-dislocations
the Lisfranc articulation is stabilized by several ligaments
Lisfranc ligament ( plantar, C1-M2)
Plantar tarsometatarsal ligament
Dorsal tarsometatarsal ligament (weak, explaining the frequent dorsal dislocation)
Intermetatarsal ligaments (no ligament between M1-M2)

Physical exam
medial plantar bruising
swelling throughout midfoot
tenderness over tarsometatarsal joint
instability test
grasp metatarsal heads and apply dorsal force to forefoot while other hand palpates the TMT joints: dorsal subluxation suggests instability. If the plantar ligaments are intact, there is no dorsal subluxation, and conservative treatment can be done.

Imaging
Xrays : AP+L
CT scan useful for diagnosis and preoperative planning
MRI can be used to confirm presence of purely ligamentous injury



dorsal subuxation
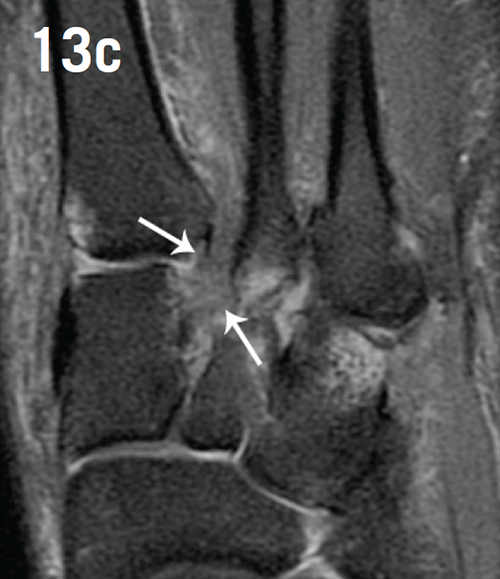
MRI showing pure ligament disruption

CT scan 3D reconstruction

Treatment
Nonoperative : cast immobilization for 8 weeks : indications
no displacement on weight-bearing and stress radiographs and no evidence of bony injury on CT (usually dorsal sprains)
certain nonoperative candidates, even if displaced
nonambulatory patients
presence of serious vascular disease
severe peripheral neuropathy instability in only the transverse plane
Operative:
open reduction and rigid internal fixation ( in bony lesions)
primary arthrodesis of the first, second and third tarsometatarsal joints (in ligamentous lesion. Generally in chronic cases)
midfoot arthrodesis: chronic lisfranc injuries that have led to advanced midfoot arthrosis and have failed conservative therapy

Chopart injury
The Chopart complex consists of two separate but interrelated joints. These include the talonavicular (TN) joint on the medial side and the calcaneocuboid (CC) joint laterally, which separate the hindfoot from the midfoot
Injury results of a low-energy twisting force applied to the plantarflexed foot
Generally a CT scan is needed.
Treatment is functionnal for pure ligamentous injuries or avulsions. short leg cast is applied for non displaced fractures.
Surgery is required for displaced fractures or dislocation.
As Lisfranc’s injury, Chopart’s lesion will frequently leads to osteoarthritis, and thus, patients will require arthrodesis (bone fusion)
This information is a brief, simple medical explanation. For exhaustive details, and before starting any kind of treatment, please refer to Dr.BAYOUD